
The marketing playbook that drove private clinic growth five years ago will not carry you through 2026. With 7.29 million patients still on NHS waiting lists as of December 2025, the patient demand flowing toward private providers is real, but so is the competition to capture it.
Every independent clinic, private GP practice, and specialist group in the country is chasing the same audience at the same moment, with tools that have grown more complex, platforms that have changed their rules, and patients who research more carefully before they commit.
This is not a prediction piece built on optimism. It is a practical guide for clinic directors who need to make sharper decisions, allocate tighter budgets, and drive measurable growth in a market that rewards precision and punishes complacency.
What follows draws from the most significant global and UK-specific healthcare marketing shifts currently reshaping patient acquisition. It adapts the ten rules now defining high-performance healthcare marketing to the specific reality of UK private clinics, GP practices, and specialist providers. It covers the compliance risks you cannot afford to ignore, the patient journey changes already underway, and the operational moves that will separate growing practices from stagnating ones.
If you run a clinic and you are responsible for revenue, this article is written for you.

⚠️ Compliance Risks Before You Start
There is no strategy without compliance. In the UK, healthcare marketing sits at the intersection of multiple regulatory frameworks, and violations in this space are not administrative inconveniences. They carry real financial, reputational, and legal consequences.
Before investing in any new channel or automation tool, clinic directors need to be clear on where the risks sit.
Data Collection and the ICO
The UK Information Commissioner’s Office (ICO) takes a strict view of health data under UK GDPR. Patient data used for marketing purposes, including browsing behaviour, form submissions, and appointment history, requires a lawful basis and, in most cases, explicit consent.
If you are running Meta Ads, Google Ads with enhanced conversions, or any server-side tracking, your data governance documentation must reflect how that data is collected, stored, and used. A poorly configured tracking pixel that passes health-related query strings back to Meta is not just a technical error. It is a potential regulatory breach.
Advertising Standards and ASA Rules
The Advertising Standards Authority (ASA) and the Medicines and Healthcare products Regulatory Agency (MHRA) both govern how private clinics advertise clinical services. Before-and-after images for certain treatments, performance claims without evidence, and misleading pricing structures are all well-documented grounds for complaints.
In 2026, with more clinics running paid social at scale, the risk of inadvertent non-compliance is rising. Every piece of creative that goes live should pass a compliance review. That process should be documented.
CQC Registration and Public Facing Claims
Any claim in a marketing asset that implies clinical quality, safety, or patient outcomes carries scrutiny if the underlying CQC registration or inspection record does not support it. Conversely, a strong CQC rating is one of the most credible trust signals a private clinic can deploy.
Using it accurately in your marketing is not just permissible; it is a competitive advantage. Misrepresenting it, or using it in contexts that imply more than the inspection found, creates both regulatory and reputational exposure.
Small missteps at the technical or creative level create larger operational consequences. Before scaling a channel, audit your compliance posture on it.

The UK Patient Journey in 2026: A Market Reshaped by NHS Pressure
Understanding where your patients come from requires understanding what has changed about how they think. In 2026, the UK patient journey to private care looks different from three years ago, in ways that directly affect where and how you should market.
The NHS waiting list, while falling from its peak, still sits at 7.29 million cases as of December 2025. Around 139,000 patients are waiting more than a year for treatment. That volume of unmet need has pushed a significant and growing segment of the UK population to seriously consider private options, many of them for the first time.
These are not lifelong private patients. They are NHS patients who have reached a point where waiting is no longer acceptable, either personally or professionally. Their research behaviour reflects that.
“The modern patient is no longer just looking for a doctor; they are looking for reassurance in a crowded market. In 2026, your digital presence is effectively your first consultation—if it doesn’t build trust instantly, the clinical relationship never begins.”
— Angelo, CEO of UpMedico
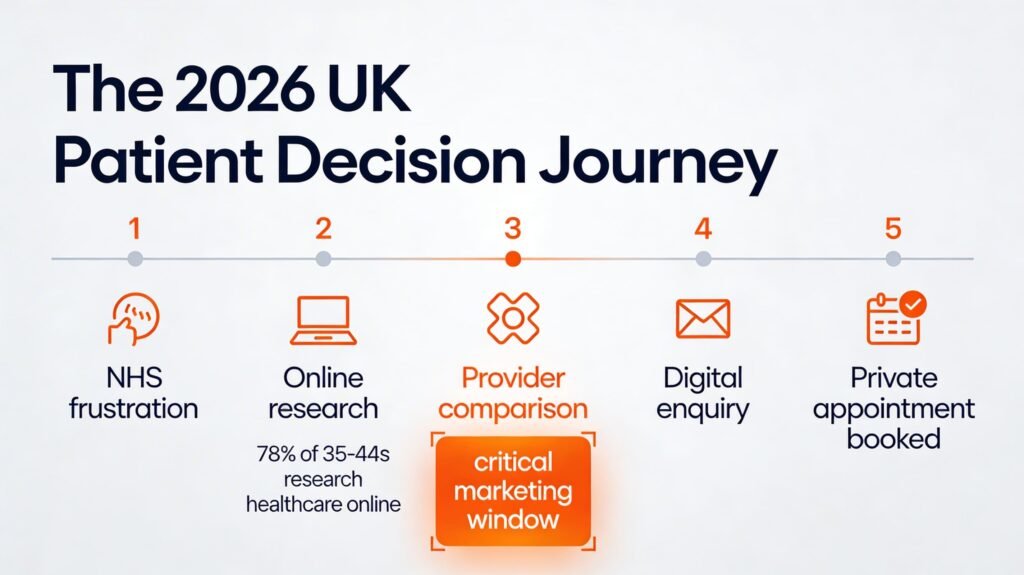
Around 70% of UK internet users now use apps or websites to access or book healthcare services, with the 35 to 44 age group showing the highest uptake at 78%. These are patients who are comparing options, reading reviews, checking credentials, and making decisions before they pick up the phone or complete a form.
Meanwhile, online consultation submissions to GP practices rose by nearly 50% between September 2024 and September 2025, a signal that digital is now the default, not the exception.
For private clinics, the strategic implication is straightforward: if your digital presence does not reach patients during the research phase, you will not be considered during the decision phase. Visibility in the moments before a patient types “private orthopaedic consultation London” or “self-pay dermatologist near me” is where patient acquisition is won or lost. The ten rules below address exactly that.
10 Marketing Rules Redefining UK Private Healthcare Growth
These are not aspirational trends. They are operational realities already shaping performance for the highest-growth private clinics and specialist groups operating in the UK.
1. Financial Accountability Is Non-Negotiable
If you cannot show the business exactly how marketing spend connects to patient volume and revenue, you will not keep control of the budget. The UK private healthcare market, valued at US $13.75 billion in 2024, is growing, but so are operating costs, insurance premiums, and competition. Clinic directors are under genuine pressure to demonstrate return on every pound spent.
The most effective marketing leaders in this environment have moved away from reporting clicks and impressions. They report scheduled appointments, attended appointments, patient lifetime value, and contribution margin by service line.
Budgets that flex monthly, based on what is performing and where the clinic can absorb new patient volume, outperform rigid annual allocations. If your marketing team is not presenting to the finance director in financial language, that needs to change now.
2. Marketing’s Mandate: Revenue, Not Responses
Leads are not the goal. Booked appointments that show up and proceed to treatment are the goal. This distinction matters practically because many UK private clinics are still measuring marketing performance on enquiry volume while ignoring conversion rates, DNA rates, and revenue per new patient.
The shift requires a shared dashboard across marketing, operations, and finance: one that tracks the full journey from first digital touchpoint through to clinical encounter and revenue collected. When everyone in the organisation uses the same numbers, budget decisions become faster and less adversarial. Marketing stops being a cost centre and starts being a growth function with a seat at the leadership table.
“We have moved past the era of vanity metrics. For a clinic director, the only marketing data that matters is what sits on the bottom line. If you cannot connect your ad spend directly to patient outcomes and revenue, you are flying blind in a storm.”
— Angelo, CEO of UpMedico
3. Unified Data Infrastructure Is the Foundation
Fragmented data is the silent killer of marketing efficiency. Many private clinics in the UK run their CRM, practice management system, phone tracking, and digital analytics in separate silos. Marketing tracks enquiries. Operations tracks appointments. Finance tracks revenue. Nobody shares a single source of truth, and the result is wasted spend, slow decisions, and internal disputes about what is actually working.
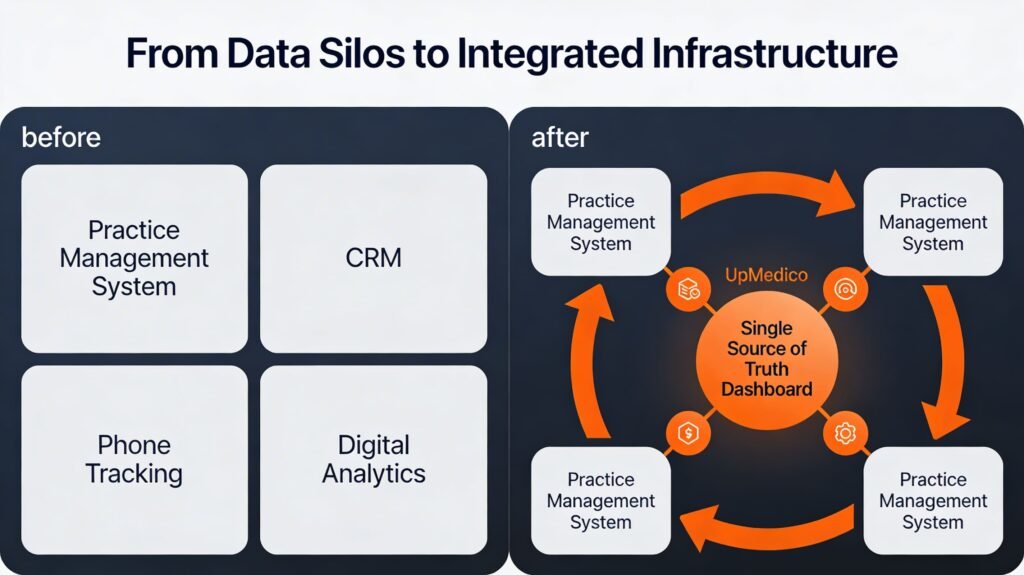
Closing that gap is as much an organisational challenge as a technical one. The practices growing fastest in 2026 are those that have invested in integration: connecting their practice management system to their CRM, passing conversion data back through server-side tracking to their advertising platforms, and building a single dashboard that reflects the patient journey from impression to revenue. It is not glamorous work, but it is the infrastructure that makes everything else possible.
4. AI as a Capability Multiplier, Within GDPR Guardrails
AI is already delivering measurable value for healthcare marketing teams that have integrated it thoughtfully. It is speeding up keyword analysis, content drafting, performance reporting, and creative iteration. It is not replacing clinical judgment, compliance review, or strategic thinking. Those remain human responsibilities.
The UK-specific consideration is data governance. Any AI tool that processes patient or prospective patient data must comply with UK GDPR. That means understanding where data is stored, whether it is processed by a third-party provider outside the UK, and whether your data processing agreements cover that use.
Clinics that adopt AI with governance frameworks in place will accelerate learning and output. Those that adopt it without those guardrails take on regulatory risk they may not have modelled.
5. Performance Creative Built for UK Patients
Generic clinic advertising fails on two levels: it does not engage the patient, and it does not train platform algorithms to find the right audience. In the UK context, this matters particularly on Meta, where the shift toward AI-driven delivery means that creative quality has become targeting. The signal the algorithm reads is the content of your ad, not the audience parameters you set.
Winning creative in 2026 does not look like a brochure. It looks like a real patient story, a clear explanation of cost and process, or a provider speaking directly about what a consultation involves. For UK private clinics, specificity builds trust: naming the consultant, the clinic location, the pathway from enquiry to treatment, and the expected timeframe.
Short-form video is increasingly dominant on paid social, with engagement rates significantly outperforming static formats in healthcare categories. Test formats continuously; let performance data decide what scales.
6. Meta Automation and What It Means for UK Clinics
Meta’s Advantage+ system has fundamentally changed how paid social works. The platform now uses AI to determine who sees your ad based on creative signals, not the audience segments you define. For UK healthcare advertisers, this creates a specific compliance challenge: you cannot rely on Meta’s targeting to exclude inappropriate audiences or to restrict delivery by geography with the precision a clinic might need.
The solution is not to avoid Meta Automation but to feed it correctly. Server-side tracking setups can pass de-identified conversion events, specifically booked appointments or qualified enquiries, back to Meta without violating UK GDPR or ICO requirements.
That teaches the algorithm what a valuable outcome looks like. Layering third-party data such as postcode-level PMI uptake or self-pay demographic signals can reintroduce geographic precision within a privacy-compliant framework. The platform automates delivery; your job is to give it the right signals.
7. The Media Mix Beyond Google Ads
Most UK private clinics allocate the majority of their digital marketing budget to paid search. The logic is understandable: search captures patients who are actively looking for a service, and intent is high. But search captures existing demand.
It does not create new demand. And in 2026, as more private providers compete for the same high-intent queries, the average cost per acquisition for UK healthcare paid search has reached approximately £48 per enquiry, with smaller, fragmented setups paying roughly double that.
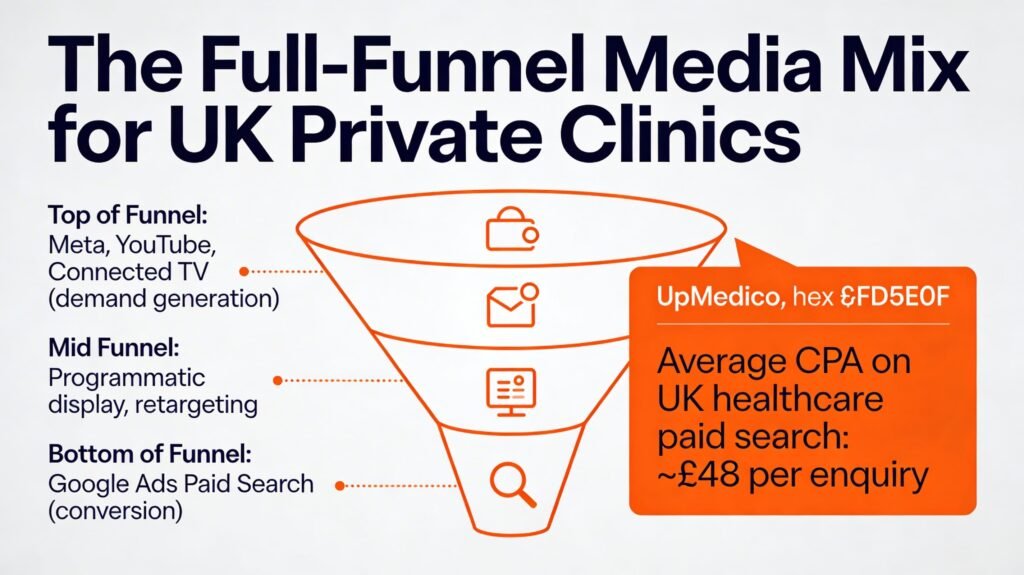
Clinics that have hit the ceiling on search performance are diversifying deliberately. Meta and YouTube address patients who are aware they have a problem but have not yet started researching providers. Connected TV reaches households with high PMI uptake in specific regions.
Programmatic display supports retargeting and reinforces brand recognition across the research journey. None of these channels replaces search. Together, they expand the pool of patients who eventually convert on it.
8. Structured Testing as Clinical Discipline
Testing in marketing should operate with the same rigour applied to clinical audit: a clear hypothesis, a defined measurement period, a pre-agreed threshold for decision, and a documented outcome. Most UK clinic marketing teams do not test at all. They run campaigns until performance declines, then change everything at once, making it impossible to identify what drove the change.
The shift toward disciplined testing does not require a large budget. Even allocating 5% of monthly spend to a structured test, whether a new channel, a new creative format, or a different landing page experience, builds institutional knowledge that compounds over time.
The clinics learning fastest are the ones winning market share, because they are making evidence-based decisions while competitors are making decisions based on habit.
9. CQC Trust Signals as a Marketing Lever
The Care Quality Commission rating is one of the most credible trust signals available to a UK private healthcare provider, and most clinics underuse it. In a market where patients are making decisions about their health, and often spending significant personal funds, a verified “Good” or “Outstanding” CQC rating provides the kind of independent validation that no amount of advertising can replicate.
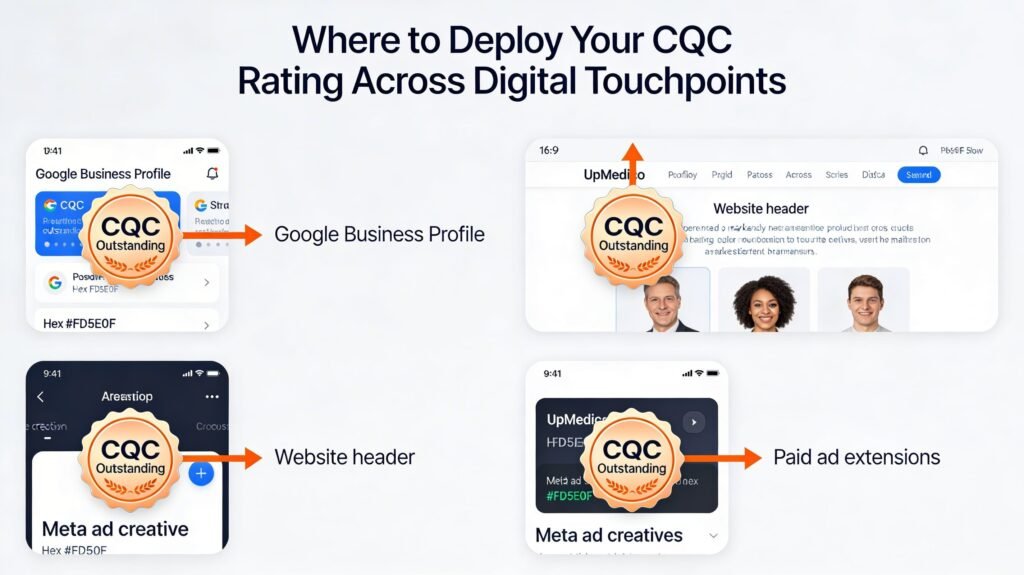
Integrating CQC status directly into digital assets, including Google Business Profiles, website headers, paid ad extensions, and Meta creative, signals credibility at the precise moment patients are comparing options.
Going further, linking to the CQC inspection report, sharing specific praise from the report in content, or featuring the CQC rating in video creative for specific service lines turns a regulatory requirement into a differentiation strategy. For clinics with strong inspection results, this is a lever that is completely free and almost entirely unused.
10. AI Search and GEO Optimisation for UK Healthcare
Around half of all Google searches now feature an AI Overview at the top of the results page, with healthcare searches among the most commonly affected categories. These AI-generated summaries pull from multiple sources and answer the patient’s question directly, reducing the need to click through to a website. For clinics that rely on organic search traffic to generate enquiries, this is a structural shift that is already affecting performance.
Optimising for AI search requires a different approach from traditional keyword ranking. Search engines and AI systems reward entities with consistent, structured, verifiable information: provider credentials, treatment descriptions, clinic locations, FAQ schema, LocalBusiness and MedicalClinic structured data markup, and accurate NAP (name, address, phone number) consistency across all directories and platforms.
For UK private clinics, this means auditing every external listing, ensuring Google Business Profiles are complete and regularly updated, and building content that answers the specific questions patients ask at each stage of their decision journey.
Targeting by ICB Region: The New Geo-Intelligence Layer
Integrated Care Boards have reshaped the NHS geography across England, and that restructuring has a direct implication for private clinic marketing. Each ICB represents a defined population health area with its own waiting time pressures, demographic profile, and concentration of self-pay or privately insured patients.
Aligning your geographic targeting to ICB boundaries, rather than broad city or county targeting, allows for a level of precision that significantly improves campaign efficiency.
A clinic in the South East, for example, can use ICB-level data to identify which specific population areas carry the highest concentrations of patients waiting more than 18 weeks for specific specialties, then weight paid search and Meta spend toward the postcodes with the highest unmet demand and the strongest private pay capacity.
This kind of geo-intelligence, built from publicly available NHS waiting time data, local PMI uptake statistics, and demographic profiling, turns broad awareness into targeted acquisition.
For multi-site groups, this approach also supports capacity-matched marketing: directing spend toward locations that have available appointment slots while reducing investment in sites already running at capacity. Marketing that drives demand into a full diary wastes budget and creates a poor patient experience. Geo-targeting at the ICB level makes it possible to align digital spend with operational reality.
Technical Infrastructure That Enables All of It
Each of the ten rules above depends on one thing: a technology stack that actually integrates. For UK private clinics, the minimum viable infrastructure in 2026 includes a practice management system that passes appointment and revenue data to the CRM, server-side tracking configured for UK GDPR compliance, a unified analytics layer that aggregates performance across all paid channels, and a Google Business Profile management system that keeps location data consistent and updated.
Beyond the basics, the clinics outperforming the market are investing in consent-mode v2 implementation across all Google properties, first-party data enrichment through email and SMS capture at the point of enquiry, and lead quality feedback loops that pass conversion outcomes back to advertising platforms without exposing health data.
The governance consideration is not a footnote. Every integration requires a data processing agreement, a privacy notice update if necessary, and a regular audit of what data is flowing where. That governance overhead is the price of operating at scale in a regulated environment.
UpMedico 2026 UK Market Outlook
From the UpMedico vantage point, the UK private healthcare marketing landscape in 2026 is defined by a single tension: significant patient demand on one side, and significant competition for that demand on the other. The UK private healthcare market was valued at US $13.75 billion in 2024 and is projected to grow to US $18.56 billion by 2033. That growth trajectory attracts capital, new entrants, and increasing consolidation among existing groups.
For independent private clinics and GP practices, the opportunity is real but time-limited. The window to build brand authority, accumulate first-party data, and establish AI-search visibility is narrowing. Large private hospital groups are investing in their digital infrastructure at pace.
The practices that move now on unified data, performance creative, CQC-led trust positioning, and GEO optimization will establish a durable advantage. Those that wait for the market to stabilise will find themselves competing against better-resourced operators with deeper data assets and stronger platform relationships.
The clinics that will grow in 2026 are those that treat marketing as a clinical discipline: structured, evidence-based, continuously improving, and directly accountable to measurable patient outcomes. That standard is not aspirational. It is the new baseline for sustainable private healthcare growth in the UK.




